
If you’ve ever stared at a blank charting screen mid-shift wondering where to even begin, you’re not alone. Nursing notes templates are one of the most searched topics among nursing students and practising RNs worldwide and for good reason. Proper documentation is not a formality. It is a clinical skill, a legal requirement, and a patient safety tool all at once.
According to the American Nurses Association, nursing documentation is a core professional and legal responsibility, not just an administrative task.
You’ll find clear definitions, step-by-step instructions, real clinical examples, and free printable templates for the three most essential nursing documentation formats: SOAP notes, SBAR notes, and the Head-to-Toe Assessment. Whether you are a first-semester student or a seasoned RN navigating a new EHR system, this guide has you covered.
📖 QUICK DEFINITION : What Are Nursing Notes Templates?
Nursing notes templates are structured documentation frameworks that guide nurses in recording patient assessments, clinical findings, communications, and care plans accurately and consistently. The three gold-standard formats are SOAP (progress notes), SBAR (handoffs and escalation), and Head-to-Toe Assessment (systematic physical examination).
Why Nursing Notes Templates Matter
Nursing documentation is one of the most time-consuming tasks nurses perform, yet it is among the most important. Research consistently shows that poor documentation contributes to adverse patient events, medication errors, and failed handoffs. Templates solve this by imposing structure at the exact moments when structure is hardest to maintain: when you’re fatigued, stretched thin, or managing multiple deteriorating patients.
Your notes are part of the official medical record and can be reviewed in malpractice cases, coroner’s inquiries, and regulatory audits. The ANA Nursing Scope and Standards of Practice outlines documentation as a fundamental expectation of every registered nurse at every level of practice.
Structured nursing notes templates also protect you legally. Your notes are part of the official medical record and can be reviewed in malpractice cases, coroner’s inquiries, and regulatory audits. As the nursing saying goes: if it wasn’t documented, it wasn’t done.
⚡ KEY STAT
Studies show structured documentation templates reduce charting time by up to 30%, decrease omission rates significantly, and improve clinical handoff accuracy, directly reducing patient harm.
Also read on How to Write SOAP Notes in Word
SOAP Notes: The Universal Nursing Notes Template
📖 DEFINITION
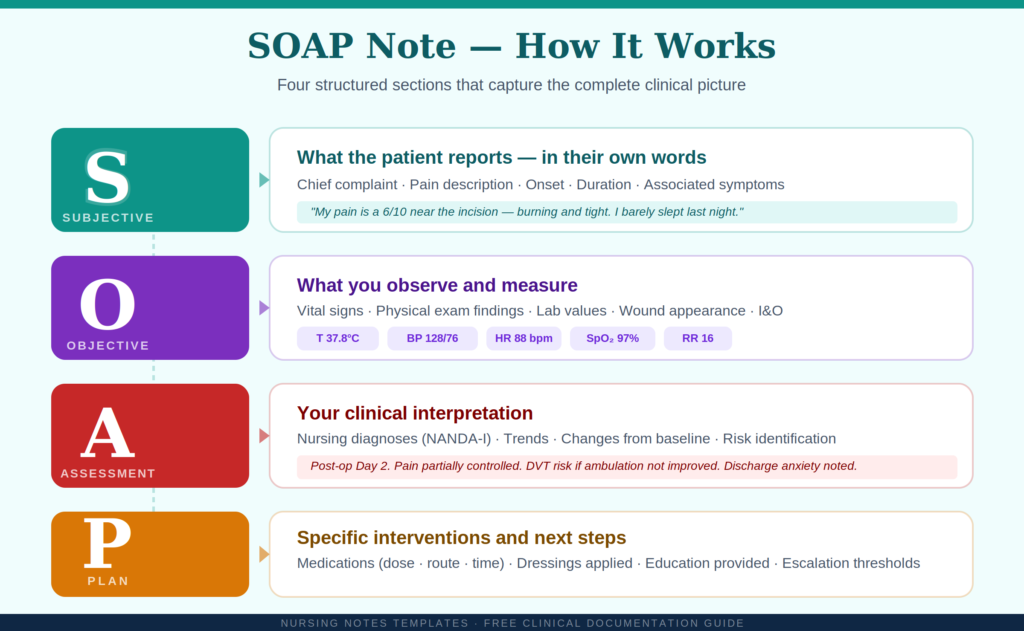
A SOAP note is a structured progress note divided into four sections: Subjective (patient’s own words), Objective (measurable data), Assessment (your clinical interpretation), and Plan (interventions and next steps). It is the most widely used nursing documentation format globally.
Originally developed in the 1960s, SOAP notes mirror the nursing process and are used in hospitals, clinics, aged care, and community settings worldwide. Nursing students can also explore guidelines for effective documentation in the OpenStax Fundamentals of Nursing textbook, which covers SOAP notes in full detail.They create a clear, logical record of your clinical reasoning for every encounter.
How to Write a SOAP Note: Step by Step
| 1 |
S — Subjective: What does the patient report?
Document the patient’s own words, chief complaint, pain description, symptoms, and relevant history they volunteer. Always use quotation marks for direct statements. |
| 2 |
O — Objective: What do you observe and measure?
Record all measurable, observable data, vital signs, physical exam findings, lab values, wound appearance, medication administered. Facts only, no interpretation. |
| 3 |
A — Assessment: What is your clinical interpretation?
Synthesise S and O into nursing diagnoses, identify trends, note changes from baseline, and document response to treatments. This is where your clinical expertise shows. |
| 4 |
P — Plan: What will you do?
List specific interventions: medications given (dose, route, time), dressings applied, education provided, physician notifications, next reassessment time, and any escalation thresholds. |
SOAP Note Example : Post-Surgical Patient
| Clinical Example: Post-Op Day 2 : Laparoscopic Appendectomy |
| S — SUBJECTIVE |
Patient states: “My pain is a 6/10 near the incision, burning and tight. I barely slept last night.” Denies nausea. Reports anxiety about discharge. |
| O — OBJECTIVE |
T 37.8°C | BP 128/76 | HR 88 | SpO₂ 97% RA | Pain 6/10. Wound: 8cm midline, edges intact, mild erythema, no exudate. BS present ×4 quadrants. IV site patent, no phlebitis. UO 680mL/8hrs. |
| A — ASSESSMENT |
Post-op Day 2. Pain partially controlled. Wound inflammation within normal post-surgical range. Mobility impaired. DVT risk if ambulation not improved. Discharge anxiety noted; education needs identified. |
| P — PLAN |
1) Paracetamol 1g IV Q6H PRN; reassess pain 45 min post-dose. 2) Physio ambulation ×3 today. 3) Wound check + dressing change 14:00. 4) SCDs in situ; LMWH 18:00. 5) Discharge education session 15:00. |
SOAP Notes: Key Takeaways:
- S = patient’s own words only, not your interpretation
- O = measurable facts only, no clinical conclusions
- A = your clinical reasoning, the most valuable section professionally
- P = specific, actionable, include doses, times, and thresholds
- Variations: SOAPIE (+Implementation, Evaluation), DAP (simplified), SOAPIER (+Revision)
- Nurses looking to earn continuing education credits can access accredited CEU courses on nursing documentation to deepen their charting skills.
SBAR Nursing Notes Template: Communication That Saves Lives
📖 DEFINITION
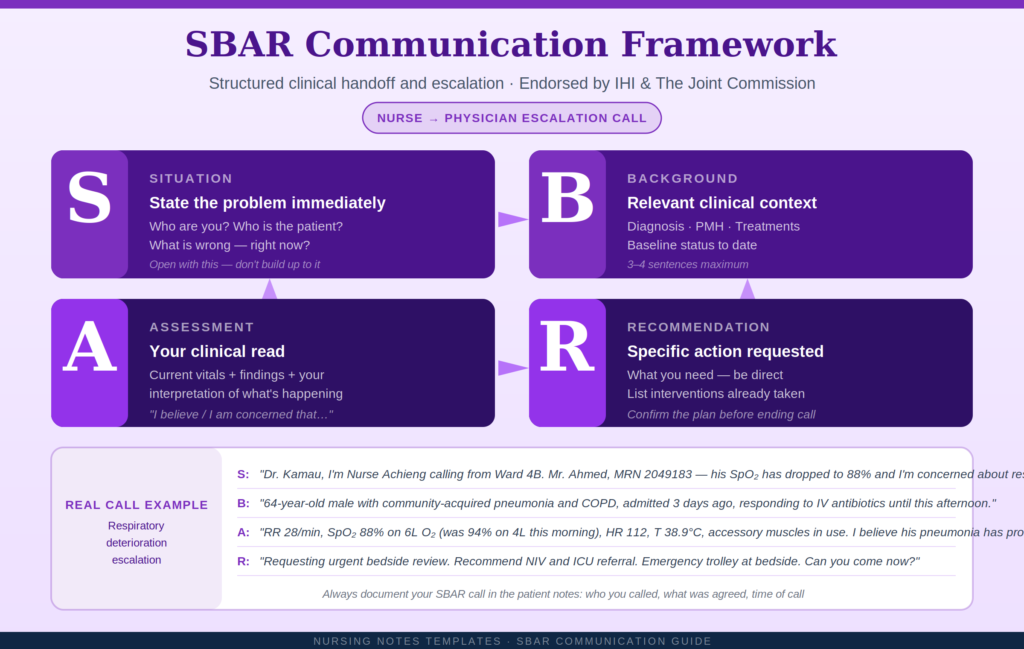
SBAR stands for Situation, Background, Assessment, Recommendation. It is a structured communication framework for clinical handoffs and escalation calls, enabling nurses to convey critical patient information concisely and safely to physicians, incoming nurses, and response teams. Endorsed by The Joint Commission and the Institute for Healthcare Improvement, SBAR was originally developed by the US Navy for life-critical communication in submarines. Healthcare adopted it because handoff communication failures are one of the most common root causes of preventable hospital harm.
Research published on PubMed Central confirms that structured handoff tools like SBAR significantly reduce adverse patient events in clinical settings.
How to Use the SBAR Template: Step by Step
| 1 |
S — Situation: State the problem immediately
Open with your name, role, patient name and MRN, and the problem — in two sentences. Don’t build up to it. The receiving clinician needs urgency confirmed within seconds. |
| 2 |
B — Background: Provide relevant context
Brief relevant history, admission diagnosis, past medical history relevant to the issue, recent treatments, and baseline status. Maximum 3–4 sentences. Don’t recite the entire chart. |
| 3 |
A — Assessment: Share your clinical read
State current vitals and observations, then your interpretation. Use ‘I believe’ or ‘I am concerned that’ to introduce your clinical judgement confidently. |
| 4 |
R — Recommendation: Be specific and assertive
State clearly what action you need. List interventions already initiated. Confirm the plan before ending the call. Be direct. don’t hint. |
SBAR Example: Respiratory Deterioration Escalation Call
| Clinical Example: Nurse-to-Physician Escalation : Ward 4B |
| S — SITUATION |
“Dr. Kamau, I’m Nurse Achieng, RN, Ward 4B. I’m calling urgently about Mr. Ahmed, MRN 2049183. His respiratory status has significantly deteriorated in the last 90 minutes, I’m concerned about impending respiratory failure.” |
| B — BACKGROUND |
64-year-old male, admitted 3 days ago with community-acquired pneumonia. Background of COPD and T2 Diabetes. Was responding to IV Amoxicillin-Clavulanate until this afternoon. ABG 12 hours ago: PaO₂ 72 mmHg. |
| A — ASSESSMENT |
Current: RR 28, SpO₂ 88% on 6L O₂ (was 94% at 08:00 on 4L), BP 108/64, HR 112, T 38.9°C. Accessory muscle use, unable to complete sentences. Coarse bilateral crackles, decreased air entry right base. I believe pneumonia has progressed, risk of acute respiratory failure. |
| R — RECOMMENDATION |
Requesting urgent bedside review. Recommend repeat CXR, ABG, high-flow nasal oxygen or NIV, and ICU referral if no improvement. Emergency trolley at bedside. Charge nurse notified. Can you come now? |
SBAR Notes : Key Takeaways:
- Open with identity and the problem, never build up to the urgency
- Background = relevant context only, 3–4 sentences maximum
- State your clinical interpretation directly: ‘I believe / I am concerned’
- Recommend a specific action, assert, don’t hint
- Document every SBAR call in the patient notes including who you spoke to
The Agency for Healthcare Research and Quality provides a comprehensive primer on handoff communication and its direct impact on patient safety outcomes.
Head-to-Toe Assessment Nursing Template
📖 DEFINITION
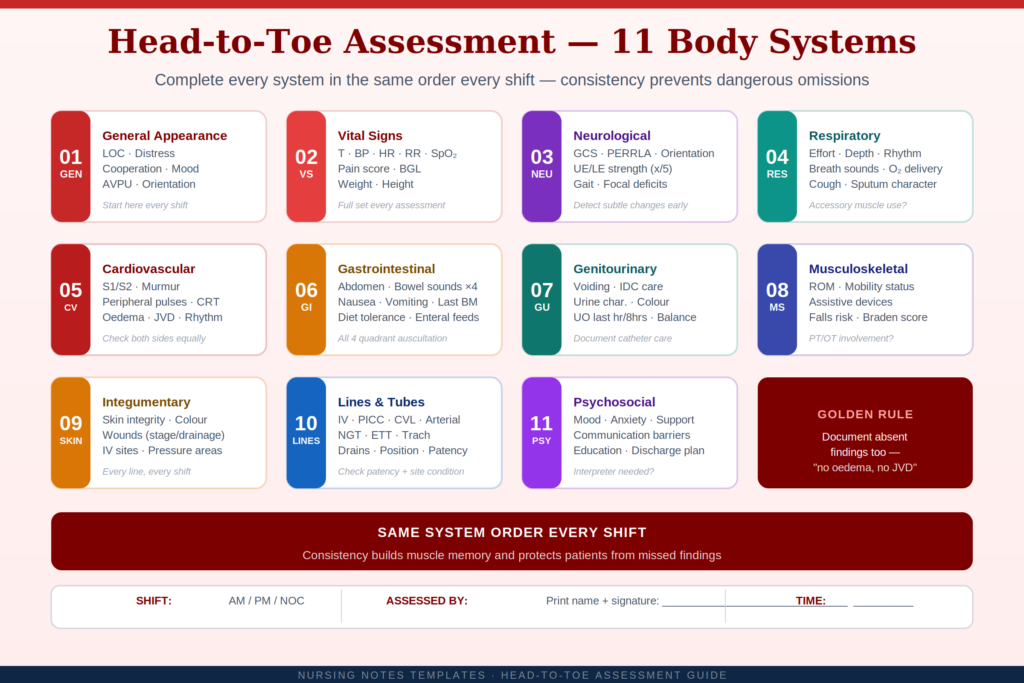
A Head-to-Toe Assessment is a systematic, body-systems-based physical examination performed at patient admission and the start of every shift. It structures how clinical data is gathered and recorded, ensuring no body system is overlooked and establishing an objective baseline for every patient.
Unlike SOAP and SBAR, which structure how findings are communicated, the Head-to-Toe template structures how those findings are collected in the first place. It is the foundation of evidence-based nursing practice across acute, critical, and long-term care settings.
The World Health Organization recognises communication failures during patient handoffs as one of the leading causes of preventable harm in healthcare globally.
Head-to-Toe Assessment Template : All Body Systems
| Head-to-Toe Assessment : Shift Documentation Template (Fill-In) |
| GENERAL |
Alert / confused / lethargic / unresponsive. Appearance: well / distressed / cachectic. Acute distress: none / present (describe). Cooperating: yes / no. |
| VITALS |
T: ___°C | BP: ___/___ | HR: ___ (reg/irreg) | RR: ___ | SpO₂: ___% (RA / O₂ ___L) | Pain: ___/10 | BGL: ___ | Wt: ___kg |
| NEURO |
GCS: E___V___M___ (___/15). PERRLA: yes/no. Orientation: person / place / time / event. UE/LE strength ___/5. Focal deficits: none / describe. |
| RESPIRATORY |
Effort: unlaboured / laboured. Breath sounds: clear / wheeze / crackles / rhonchi (site: ___). Accessory muscles: no / yes. Cough: none / productive / non-productive. |
| CARDIOVASCULAR |
S1/S2: regular / irregular. Murmur: none / grade ___. Peripheral pulses: strong / weak / equal. CRT: <2s />2s. Oedema: none / pitting ___ (site). Rhythm: ___. |
| GASTROINTESTINAL |
Abdomen: soft / rigid / distended. Tenderness: none / site ___. BS: ×4 / hypoactive / absent. Last BM: ___. Nausea / vomiting: no / yes. Diet: tolerating / NPO. |
| GENITOURINARY |
Voiding: independently / IDC (type/size ___, care given). Urine: clear / cloudy / haematuria. UO last hr: ___ mL. Dysuria: no / yes. |
| MUSCULOSKELETAL |
ROM: intact / limited (site: ___). Mobility: independent / assisted (device: ___) / dependent / bed-bound. Falls risk score: ___. Braden score: ___. |
| INTEGUMENTARY |
Skin: intact / impaired. Colour: pink / pale / jaundiced / cyanotic. Wounds: none / describe (site, size, stage, drainage, dressing). IV site: patent / phlebitis. |
| LINES & TUBES |
IV access: PIV / PICC / CVL, site, condition, date. NGT: position confirmed, pH ___. Drains: type, output, colour. Trach / ETT: details. |
| PSYCHOSOCIAL |
Mood: appropriate / anxious / depressed. Communication barrier: none / language / hearing. Support: family present / absent. Education provided: yes (topic: ___) / no. |
Head-to-Toe Assessment : Key Takeaways:
- Use the same system order every shift to build muscle memory and prevent omissions
- Document what is absent as well as what is present (‘no oedema, no JVD’)
- Timestamp all assessments — legally significant, especially for deterioration events
- Compare findings to the previous shift’s note to detect subtle changes early
- Every line, tube, and drain must be inspected and documented every shift
For a quick bedside reference, download the nursing documentation pocket card from Nursing Center, a practical summary of documentation do’s and don’ts.
Choosing the Right Nursing Notes Template
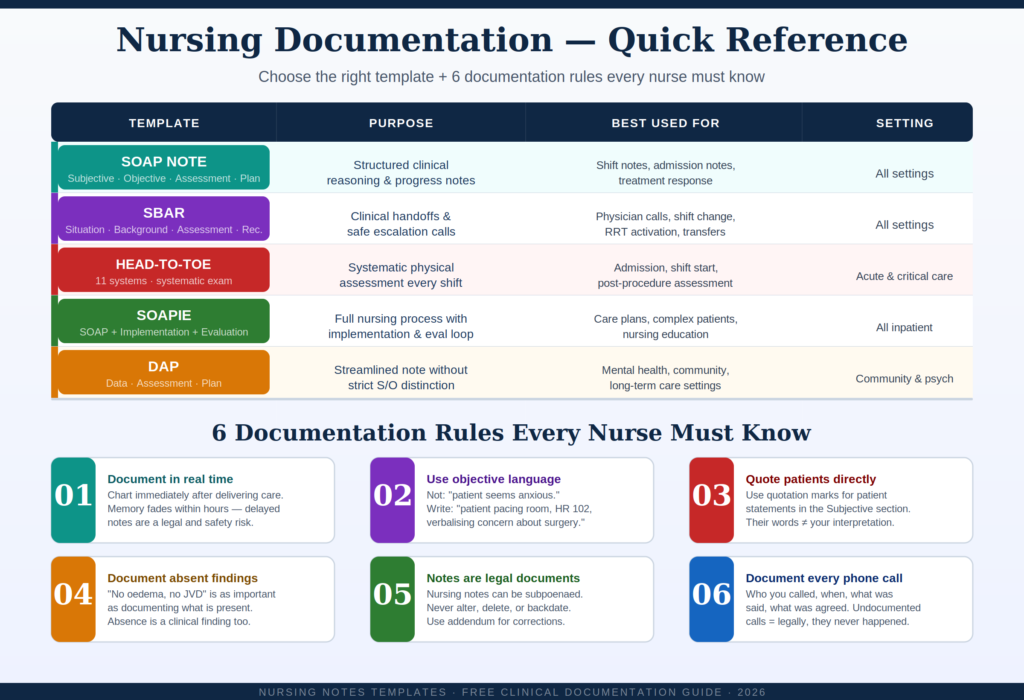
Each nursing notes template serves a different clinical purpose. Use this quick reference to choose the right format every time:
| Template |
Primary Purpose |
Best Used For |
Setting |
| SOAP |
Structured progress notes |
Shift notes, admission notes, treatment response |
All settings |
| SBAR |
Clinical communication |
Physician calls, shift handoffs, RRT activation |
All settings |
| Head-to-Toe |
Systematic physical assessment |
Admission, shift start, post-procedure |
Acute & critical care |
| SOAPIE |
Full nursing process |
Care plans, complex patients |
All inpatient |
| DAP |
Simplified progress note |
Mental health, community care |
Community & psych |
2026 Trends: Digital & AI Nursing Documentation
Nursing documentation is evolving rapidly. Here’s what’s changing in 2026:
- AI Ambient Charting: Tools like Nuance DAX auto-draft SOAP notes from your assessments , nurses review and sign.
- Voice-to-Text EHR: Clinical speech recognition reduces bedside documentation time by 40–60% in pilot hospitals.
- Mobile-First Charting: Real-time documentation at the bedside via smartphone EHR apps, eliminating end-of-shift backlogs.
- Predictive Alerts: AI embedded in EHRs flags sepsis, deterioration, and falls risk directly in the nursing flowsheet.
IMPORTANT
AI drafts reflect data patterns, they do not replace clinical judgement. Your signature on any note is a legal attestation of accuracy. Always review and personalise AI-generated documentation before signing.
Frequently Asked Questions: Nursing Notes Templates
Hospitals accredited by The Joint Commission are required to meet specific documentation standards as part of their national performance goals.
Q: What is a SOAP note in nursing?
A: A SOAP note is a structured nursing progress note divided into Subjective (patient’s reported symptoms), Objective (measurable clinical findings), Assessment (nurse’s clinical interpretation), and Plan (interventions and next steps). It is the most widely used nursing documentation format globally and is accepted across hospitals, clinics, and community care settings.
Q: What is the difference between SOAP notes and SBAR?
A: SOAP notes are used to document clinical reasoning and assessments in the patient’s chart (a charting tool). SBAR is a communication framework used to convey patient information during handoffs and escalation calls (a communication tool). Both can be used in the same clinical encounter, gather data with a Head-to-Toe assessment, chart it with SOAP, then communicate it via SBAR.
Q: What should a nursing head-to-toe assessment include?
A: A complete head-to-toe nursing assessment covers: general appearance and vital signs, neurological status (GCS, orientation, pupils, motor strength), respiratory (breath sounds, effort, oxygen), cardiovascular (heart sounds, pulses, oedema), gastrointestinal (bowel sounds, abdomen, last BM), genitourinary (voiding, urine, catheter care), musculoskeletal (mobility, ROM, falls risk), integumentary (skin integrity, wounds, IV sites), all lines and tubes, and psychosocial status (mood, support, education).
Q: Are nursing notes legal documents?
A: Yes. Nursing notes are part of the official medical record and are legally admissible in court proceedings, malpractice cases, regulatory audits, and coroner’s inquiries. Always document accurately and in real time. Never alter, delete, or backdate records, corrections must be made via single line-through (paper) or addendum (EHR). Signing a note is a legal attestation of its accuracy.
Q: How often should nursing notes be written?
A: Documentation frequency varies by acuity: ICU patients require documentation every 1–2 hours; medical-surgical ward patients require a full shift assessment at the start of each shift and progress notes every 4–8 hours or with any clinical change; long-term care requires weekly notes plus documentation of any incidents. Always document immediately for any patient deterioration, medication administration, adverse event, or physician notification.
Q: Can nurses use AI tools to write nursing notes?
A: AI-assisted charting tools (such as ambient AI listeners built into Epic or Nuance DAX) are increasingly available and can reduce documentation time significantly. However, nurses must review and personally authenticate every AI-generated note before signing, your signature is a legal attestation of accuracy. Never use general consumer AI tools (chatbots) for patient documentation, as this raises serious data privacy and compliance concerns.
Q: Where can I download free nursing notes templates?
A: You can print the SOAP, SBAR, and Head-to-Toe templates included in this article directly from your browser (use Ctrl+P or Cmd+P → Save as PDF). Many nursing schools and professional nursing bodies also offer downloadable templates. Always verify that any template you use meets your institution’s documentation policy requirements.
Final Thoughts: Documentation Is a Clinical Skill
Nursing notes templates are not bureaucratic checkboxes. They are the professional language of nursing — the mechanism through which your clinical judgement becomes visible, shareable, and legally defensible. Mastering SOAP notes, SBAR communication, and Head-to-Toe assessments will make you a safer, faster, and more confident nurse.
Start practising these formats today. If you found this guide helpful, bookmark it, share it with your cohort, and leave a comment below with the template you find most challenging, we read every response.
📌 QUICK RECAP : The 3 Essential Nursing Notes Templates
SOAP Notes → For structured progress notes and clinical reasoning (all settings)
SBAR → For handoffs, escalation calls, and inter-professional communication (all settings)
Head-to-Toe Assessment → For systematic physical examination and shift documentation (acute & critical care)








 Evan John
Evan John