Writing a nursing care plan can feel overwhelming for many student nurses, especially during clinical rotations and exams. A well-structured nursing care plan template for students helps simplify the process by organizing patient assessment, nursing diagnoses, goals, interventions, and evaluation in a clear format. You will learn how to create effective nursing care plans, avoid common mistakes, and use practical examples to improve your clinical documentation skills and patient care.
Why Every Nursing Student Needs a Solid Care Plan Template
If you’re a nursing student, you’ve probably heard your clinical instructor say it more than once: “Where’s your care plan?” Nursing care plans are the backbone of patient-centered care, and learning how to write them effectively is one of the most critical skills you’ll develop during your training.
But here’s the problem most students stare at a blank template and don’t know where to start.
This guide walks you through everything you need to know about nursing care plan templates: what they are, why they matter, what each section means, and how to complete one confidently. Whether you’re in your first clinical rotation or preparing for the NCLEX, this resource is built for you.
What Is a Nursing Care Plan?
A nursing care plan (NCP) is a formal document that outlines a patient’s health needs, nursing diagnoses, expected outcomes, and the specific interventions nurses will use to achieve those outcomes. It serves as a communication tool between the nursing team, other healthcare providers, and the patient.
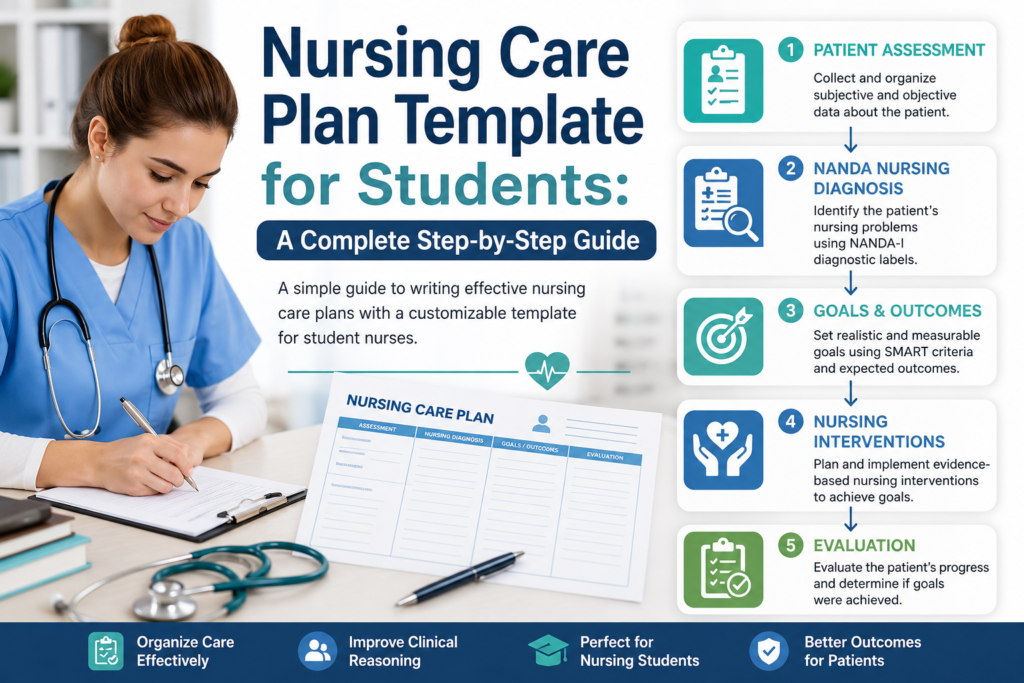
Care plans are rooted in the nursing process a five-step framework that forms the foundation of modern nursing practice:
- Assessment – Collecting patient data
- Diagnosis – Identifying health problems
- Planning – Setting measurable goals
- Implementation – Carrying out nursing interventions
- Evaluation – Measuring outcomes and adjusting the plan
A good care plan template mirrors this process, keeping your thinking organized and your documentation professional.
The Standard Nursing Care Plan Template: Section by Section
Here is a breakdown of the core sections found in most nursing care plan templates used in academic and clinical settings.
1. Patient Information
What to include:
- Patient’s age, gender, and admission date
- Primary diagnosis or reason for admission
- Relevant medical history, allergies, and current medications
Why it matters: This section contextualizes everything that follows. A 72-year-old post-operative patient requires a very different care plan than a 25-year-old admitted for a first asthma episode.
Student tip: Never copy this section from the chart without reading it. Understanding the patient’s full picture will make your nursing diagnoses much sharper.
2. Nursing Assessment
This is the data-gathering phase. Your assessment should cover both subjective data (what the patient tells you) and objective data (what you observe and measure).
Subjective data examples:
- “I can’t catch my breath when I walk to the bathroom.”
- “My pain is a 7 out of 10.”
Objective data examples:
- SpO₂: 91% on room air
- Respiratory rate: 26 breaths per minute
- Bilateral crackles on auscultation
Assessment categories to cover:
- Airway and breathing
- Circulation and cardiovascular status
- Neurological status (level of consciousness, orientation)
- Pain assessment
- Skin integrity
- Nutrition and hydration
- Elimination
- Psychosocial and emotional status
- Safety and fall risk
- Patient/family knowledge and readiness to learn
Student tip: Use a head-to-toe or body systems framework to make sure you don’t miss anything. Many clinical facilities use structured tools like the Gordon’s Functional Health Patterns model.
3. Nursing Diagnosis
This is often the hardest section for students and the one that matters most. The nursing diagnosis is different from a medical diagnosis. It focuses on the human response to illness, not the disease itself.
Nursing diagnoses follow the NANDA-I (North American Nursing Diagnosis Association International) taxonomy. Each diagnosis has three parts:
PES Format:
- P – Problem (the nursing diagnosis label)
- E – Etiology (related to / “as evidenced by” causative factors)
- S – Signs and Symptoms (as evidenced by / defining characteristics)
Example:
Impaired Gas Exchange related to alveolar-capillary membrane changes as evidenced by SpO₂ of 91%, respiratory rate of 26, and patient-reported shortness of breath.
Common NANDA nursing diagnoses for students to know:
- Acute Pain
- Risk for Infection
- Impaired Physical Mobility
- Deficient Knowledge
- Ineffective Breathing Pattern
- Imbalanced Nutrition: Less Than Body Requirements
- Anxiety
- Risk for Falls
Student tip: Prioritize your diagnoses using Maslow’s Hierarchy of Needs — physiological needs (like breathing and circulation) always come before psychological ones.
4. Goals and Expected Outcomes
Once you’ve identified your nursing diagnosis, you need to set clear, measurable goals. These are written from the patient’s perspective, not the nurse’s.
All goals should be SMART:
- Specific
- Measurable
- Achievable
- Relevant
- Time-bound
Short-term goal example:
Patient will report pain level of 3 or less on a 0–10 scale within 1 hour of analgesic administration.
Long-term goal example:
Patient will demonstrate correct use of incentive spirometer and maintain SpO₂ above 95% on room air by discharge.
Student tip: Avoid vague goals like “patient will feel better.” Every goal must include a measurable indicator and a time frame.
5. Nursing Interventions
Nursing interventions are the specific actions you will take to help the patient achieve their goals. Interventions fall into three categories:
- Independent interventions – Actions within the nurse’s scope of practice (e.g., repositioning, patient education, monitoring vital signs)
- Dependent interventions – Actions requiring a physician’s order (e.g., administering medications, performing procedures)
- Collaborative interventions – Actions carried out with other healthcare team members (e.g., physiotherapy, dietary consultation)
Example interventions for Impaired Gas Exchange:
- Monitor SpO₂ continuously and report readings below 92% to the physician.
- Elevate the head of the bed to 30–45 degrees to facilitate lung expansion.
- Encourage use of incentive spirometer every 1–2 hours while awake.
- Administer prescribed bronchodilators as ordered and document response.
- Teach the patient diaphragmatic breathing techniques.
Student tip: Always include a rationale for each intervention in academic care plans. This demonstrates your clinical reasoning and shows your instructor that you understand why you’re doing what you’re doing.
Also read on Common Nursing Diagnoses and Interventions List: A Complete Clinical Reference
6. Evaluation
The final section is where you determine whether your interventions worked. You revisit your goals and honestly assess whether the patient met them, partially met them, or did not meet them.
Evaluation format:
Goal met / Partially met / Not met. Patient’s SpO₂ improved to 96% on room air after 4 hours. Patient demonstrates correct use of incentive spirometer. Continue current plan.
If goals are not met, the evaluation section should explain why and propose revisions to the care plan.
Student tip: Evaluation is not a formality it’s where critical thinking shines. Don’t just write “goal met.” Explain what you observed, what changed, and what you would do differently.
Quick-Reference Nursing Care Plan Template
| Section |
Key Question |
What to Write |
| Patient Information |
Who is this patient? |
Age, diagnosis, history, meds |
| Assessment |
What data did I collect? |
Subjective + objective findings |
| Nursing Diagnosis |
What is the health problem? |
NANDA label + etiology + signs |
| Goals/Outcomes |
What do I want to achieve? |
SMART goals, patient-focused |
| Interventions |
What will I do? |
Independent, dependent, collaborative |
| Evaluation |
Did it work? |
Goal met/not met + reasoning |
5 Common Mistakes Nursing Students Make on Care Plans
- Confusing medical and nursing diagnoses. “Pneumonia” is a medical diagnosis. “Impaired Gas Exchange” is a nursing diagnosis.
- Writing vague goals. “Patient will breathe better” is not measurable. Attach a number and a time frame.
- Listing interventions without rationale. In academic settings, always explain why you’re implementing each intervention.
- Skipping the evaluation. This is where you demonstrate critical thinking never rush it.
- Prioritizing incorrectly. Always address life-threatening physiological issues before psychosocial or educational diagnoses.
Final Thoughts
Mastering the nursing care plan template is not just an academic exercise it’s the foundation of safe, effective, evidence-based nursing practice. Every section of the care plan trains you to think like a nurse: systematically, critically, and always with the patient at the center.
Use the template and guidelines in this post as your starting framework, adapt it to each patient’s unique needs, and always ask yourself: “What does this patient need from me right now?”
The more care plans you write, the more natural the clinical reasoning becomes and that’s exactly the nurse your future patients need.







 Evan John
Evan John