Staring at a blank care plan worksheet at midnight before clinical every nursing student knows that feeling. You understand the theory, you have read the textbook, but translating real patient data into a structured, professional nursing care plan template for students still feels like solving a puzzle with missing pieces.
This guide changes that completely. You will get a clear, ready-to-use nursing care plan template for students, a step-by-step breakdown of each section, real clinical examples, practical tips that work in hospital settings, and a full FAQ section optimized for quick reference. Whether you are in your first semester or finishing your final year, this resource will make care planning faster, cleaner, and far more effective.
The nursing care plan template for students shared in this guide follows the most current NANDA-I taxonomy, aligns with evidence-based practice standards, and meets the expectations of clinical faculty across nursing programs worldwide.
What Is a Nursing Care Plan and Why Does It Matter?
A nursing care plan is a formal written document that guides individualized, patient-centered care. It organizes your clinical thinking so that every member of the healthcare team nurses, physicians, therapists, and aides understands the patient’s needs, goals, and the specific interventions planned to achieve positive outcomes.
For nursing students, care plans serve an even deeper purpose. They train your clinical reasoning. Writing a care plan forces you to connect your assessment findings to nursing diagnoses, then map those diagnoses to realistic interventions and measurable, time-bound goals. That thinking process is exactly the skill you will use every single day as a licensed nurse in any clinical setting.
Using a reliable nursing care plan template for students consistently helps you:
- Stay organized during hectic clinical days and high-acuity patient assignments
- Avoid missing critical components that faculty and preceptors look for
- Submit assignments that meet or exceed faculty expectations and rubric requirements
- Build professional documentation habits that translate directly into registered nursing practice
- Develop the confidence to prioritize patient needs accurately under pressure
The ADPIE Framework: The Backbone of Every Care Plan
Every effective nursing care plan follows the ADPIE nursing process. This five-step framework is the universal language of professional nursing and the foundation of every nursing care plan template for students used in accredited programs.
- Assessment — Collect comprehensive subjective and objective patient data
- Diagnosis — Identify nursing diagnoses using current NANDA-I terminology
- Planning — Set SMART goals and measurable expected outcomes
- Implementation — List evidence-based nursing interventions with clinical rationale
- Evaluation — Measure whether stated goals were achieved and revise as needed
Understanding ADPIE deeply is non-negotiable before you fill in any nursing care plan template for students. It is the logic that makes your care plans clinically sound, defensible, and genuinely useful, rather than just academic paperwork to submit and forget.
Nursing Care Plan Template for Students: Complete Format
Below is a comprehensive nursing care plan template for students that covers every required section in the correct order. Use this as your master format for all clinical assignments, hospital rotations, and simulation lab experiences.
Section 1: Patient Assessment Data
Assessment is always the first step. Gather both types of data before writing a single diagnosis.
Subjective Data (What the patient says):
- Chief complaint in the patient’s own words — example: ‘I feel short of breath when I walk to the bathroom’
- Pain description: location, quality, severity (0-10 scale), onset, duration, and aggravating or relieving factors
- Patient-reported symptoms, concerns, fears, and psychosocial information
Objective Data (What you observe and measure):
- Vital signs: Blood Pressure, Heart Rate, Respiratory Rate, SpO2, Temperature, Pain Score
- Physical assessment findings: breath sounds, skin color and integrity, pupil response, bowel sounds, edema, motor strength
- Laboratory values and diagnostic results: CBC, BMP, ABGs, chest X-ray, EKG findings
- Current medications, allergies, and relevant medical and surgical history
- Functional assessment: ability to perform ADLs, mobility status, fall risk score
Pro Tip: Always separate subjective from objective data clearly in your nursing care plan template for students. Mixing these two categories is one of the most common points deducted on care plan assignments and clinical evaluations.
Section 2: Nursing Diagnosis (NANDA Format)
Use the three-part NANDA diagnostic statement for actual nursing diagnoses:
Problem related to Etiology as evidenced by Signs and Symptoms
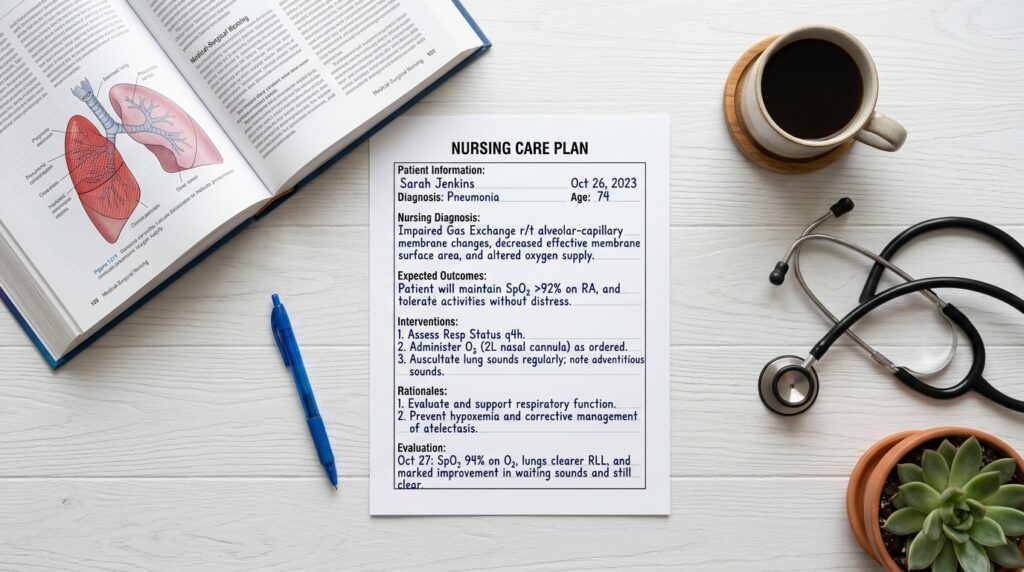
Example: Impaired Gas Exchange related to alveolar-capillary membrane changes as evidenced by SpO2 of 89% on room air, use of accessory muscles, and patient-reported dyspnea on exertion.
For risk diagnoses, only two parts are used because the problem has not yet occurred:
Risk for Infection related to presence of central venous catheter and immunosuppressive therapy.
For each care plan, prioritize diagnoses using Maslow’s Hierarchy of Needs. Always address physiological problems before psychosocial ones, unless safety is at immediate and imminent risk. This prioritization demonstrates clinical judgment and earns higher scores on evaluations.
Section 3: Goals and Expected Outcomes (NOC)
Goals in your nursing care plan template for students must always be written as SMART objectives: Specific, Measurable, Achievable, Realistic, and Time-bound. Vague goals are one of the biggest weaknesses in student care plans.
Short-Term Goal Example: The patient will maintain SpO2 greater than or equal to 94% on room air within 24 hours of implementing nursing interventions.
Long-Term Goal Example: The patient will independently demonstrate the pursed-lip breathing technique with correct form and rate before discharge from the medical-surgical unit.
Write at least one short-term and one long-term goal per nursing diagnosis. Both goals must be patient-focused, not nurse-focused. The subject of every goal statement is always the patient, not the nurse.
Section 4: Nursing Interventions (NIC) with Rationale
This is the most detailed and heavily graded section of any nursing care plan template for students. For each intervention, always provide a specific clinical rationale grounded in evidence-based practice. Faculty and clinical instructors look for this connection every time.
| Nursing Intervention |
Clinical Rationale |
| Position patient in High-Fowler’s (90 degrees) |
Maximizes lung expansion and reduces work of breathing |
| Administer prescribed supplemental oxygen per order |
Corrects hypoxemia and improves tissue oxygenation |
| Monitor SpO2 every 2 hours and document findings |
Allows early detection of respiratory deterioration |
| Teach pursed-lip breathing technique |
Slows respiratory rate and improves gas exchange efficiency |
| Encourage fluid intake of 2-3L/day unless contraindicated |
Thins secretions and facilitates expectoration |
| Auscultate breath sounds every nursing shift |
Tracks changes in airway status and identifies complications |
| Elevate head of bed and reposition every 2 hours |
Prevents atelectasis and promotes comfort |
| Administer bronchodilators as prescribed |
Relaxes airway smooth muscle and improves airflow |
Include at least five to six interventions per diagnosis. Make sure to include a mix of independent interventions (actions nurses perform autonomously), dependent interventions (physician-ordered actions nurses carry out), and collaborative interventions (coordinated with the interdisciplinary team including physical therapy, respiratory therapy, dietitians, and social work).
Section 5: Evaluation
Evaluation closes the care plan loop. After implementing your interventions, formally evaluate whether the patient met the stated goals within the established time frame. This section demonstrates your ability to think critically and adapt care based on patient response.
- Goal Met: SpO2 maintained at 96% for 12 hours; patient denies shortness of breath at rest and demonstrates correct pursed-lip breathing technique.
- Goal Partially Met: Patient can demonstrate pursed-lip breathing but still reports dyspnea with moderate exertion. Continue current interventions and reassess in 12 hours.
- Goal Not Met: Patient SpO2 remains below 92% despite interventions. Notify physician, reassess contributing factors, revise interventions, and update care plan accordingly.
Evaluation is not just a checkbox at the bottom of the page. It is where your deepest clinical thinking happens. A strong evaluation section shows faculty that you understand nursing as a dynamic, responsive process.
Common Nursing Diagnoses Used in Student Care Plans
Using a nursing care plan template for students becomes significantly easier when you are familiar with the most frequently used NANDA-I diagnoses across clinical rotations:
- Acute Pain related to surgical incision as evidenced by pain rating 8/10 and guarding behavior
- Risk for Infection related to invasive line insertion and compromised skin integrity
- Deficient Knowledge related to new Type 2 diabetes diagnosis as evidenced by patient questions and inability to self-administer insulin
- Impaired Physical Mobility related to left hip fracture as evidenced by inability to bear weight and limited range of motion
- Anxiety related to upcoming cardiac catheterization as evidenced by patient reports of fear and observed restlessness
- Imbalanced Nutrition: Less Than Body Requirements related to nausea and anorexia as evidenced by weight loss of 8 lbs in two weeks
- Risk for Falls related to altered gait, muscle weakness, and sedating medications
- Impaired Urinary Elimination related to urinary catheter as evidenced by dark, concentrated output
Each of these diagnoses can be inserted directly into the nursing care plan template for students shared above and fully customized to match your specific patient’s clinical presentation and assessment data.
Also read on Sample Nursing Care Plan for Hypertension: A Complete 2026 Guide
Pro Tips to Score High on Care Plan Assignments
Instructors and clinical evaluators grade care plans on three core qualities: specificity, accuracy, and evidence base. Here is how to consistently produce care plans that stand out.
1. Be Patient-Specific in Every Section
Generic care plans fail consistently. Use your actual assessment data throughout every section of your nursing care plan template for students. ‘Pain rated 7 out of 10 in the right lower quadrant, described as sharp and constant, worsened with movement’ is infinitely more valuable than simply writing ‘patient reports pain.’ Specificity is the mark of clinical competence.
2. Use Current NANDA-I Taxonomy
Always reference the most recent edition of NANDA International approved diagnoses. Outdated, discontinued, or incorrectly formatted nursing diagnoses cost points immediately on any assignment and reflect poorly in clinical settings. When in doubt, verify with your NANDA-I Nursing Diagnoses textbook.
3. Include Evidence-Based Rationale for Every Intervention
Never write an intervention without explaining why it is clinically appropriate. Cite your nursing fundamentals textbook, clinical practice guidelines from organizations like the American Nurses Association or the CDC, or peer-reviewed nursing journals when explaining the rationale for your chosen interventions. This demonstrates that your care plan is grounded in science, not intuition.
4. Prioritize Diagnoses Correctly Using Maslow
Never place a comfort or psychosocial diagnosis above an airway, breathing, circulation, or safety diagnosis. Show Maslow’s Hierarchy of Needs in your ordering clearly. This prioritization is one of the most direct demonstrations of clinical judgment in your entire nursing care plan template for students.
5. Match Every Intervention Directly to a Goal
Each intervention should logically and directly connect to at least one of your stated goals. If an intervention does not connect to any goal, remove it or rewrite your goals. Mismatched interventions and goals are a common source of lost points that are easy to avoid with careful review before submission.
How to Download and Use This Template
To use this nursing care plan template for students effectively in your clinical rotations and academic submissions:
- Save the format sections above into a Word document or Google Doc with proper spacing and headings
- Create a professional header with patient initials, age, primary medical diagnosis, clinical date, and your full name
- Fill in each section in the presented order: Assessment, then Diagnosis, then Goals, then Interventions, then Evaluation
- Cross-reference every section with your assigned faculty rubric before finalizing
- Review the complete document for specificity — replace any generic language with patient-specific clinical data
- Submit in the required format: printed, digital PDF, or Word document as directed by your program
Many nursing programs now accept digital submissions through learning management systems. Google Docs and Microsoft Word are both excellent tools for organizing this nursing care plan template for students clearly. Consider creating a folder system on your device to store care plans from each rotation as a personal clinical portfolio.
Frequently Asked Questions
These questions are optimized for Google featured snippets and cover the most common points of confusion nursing students have about care planning.
Q1: What should be included in a nursing care plan template for students?
A complete nursing care plan template for students must include five core sections: patient assessment data covering both subjective and objective findings, a properly formatted NANDA-I nursing diagnosis, SMART goals and measurable expected outcomes, evidence-based nursing interventions with clinical rationale for each, and a formal evaluation of whether goals were achieved within the stated time frame. These five sections follow the ADPIE nursing process framework and are required in virtually every accredited nursing program worldwide.
Q2: How many nursing diagnoses should a student care plan include?
Most nursing school assignments require between one and three nursing diagnoses per care plan, though some programs specify an exact number. Always prioritize diagnoses using Maslow’s Hierarchy of Needs, addressing physiological and safety needs before psychosocial concerns. Confirm the expected number with your instructor’s rubric before beginning your assignment, as requirements vary significantly across programs and clinical settings.
Q3: What is the correct NANDA nursing diagnosis format?
The standard three-part NANDA-I format for actual nursing diagnoses is: Nursing Diagnosis related to Etiology as evidenced by Signs and Symptoms. For example: Acute Pain related to tissue damage from abdominal surgery as evidenced by patient rating pain 8 out of 10, guarding behavior, and facial grimacing. Risk diagnoses do not include the ‘as evidenced by’ component because the problem has not yet occurred. Only two parts are used: Risk for (diagnosis) related to (risk factors).
Q4: Can I use the same nursing care plan template for different clinical rotations?
Yes. The nursing care plan template for students shared in this guide is universal and works effectively across medical-surgical, pediatric, obstetric, psychiatric, community health, and critical care rotations. The format remains the same throughout all clinical settings. You simply replace the patient data, nursing diagnoses, goals, and interventions with content that is appropriate and specific to each specialty and patient presentation.
Q5: What is the difference between a nursing diagnosis and a medical diagnosis?
A medical diagnosis identifies a specific disease, condition, or pathology determined by a physician, such as community-acquired pneumonia or Type 2 diabetes mellitus. A nursing diagnosis identifies the patient’s human response to that medical condition or to life processes, as determined by the registered nurse. For example, the nursing diagnosis for a patient with pneumonia might be Impaired Gas Exchange or Ineffective Airway Clearance. Nursing care plans are always built around nursing diagnoses, not medical diagnoses, because nursing’s scope focuses on the patient’s response and functional outcomes.
Conclusion
A strong nursing care plan template for students is far more than an academic requirement. It is the foundation of safe, organized, evidence-based, patient-centered care. When you master the format, deeply understand the ADPIE process, and consistently practice writing specific, rationale-driven care plans, you build the clinical reasoning skills that define excellent, competent, compassionate nurses throughout their careers.
Use the template in this guide for every clinical rotation. Customize every section to your actual patient. Connect your interventions back to measurable, time-bound goals. And evaluate your outcomes honestly, because that reflection is where true clinical growth happens.
The nursing students who produce the best care plans are not necessarily the ones who studied the hardest in the classroom. They are the ones who practiced the format consistently, stayed patient-specific, and never stopped asking ‘why’ behind every intervention they wrote.
Ready to level up your nursing studies? Bookmark this guide, save the template, and share it with your entire cohort. Explore our other nursing student resources from complete NANDA diagnosis lists to medication administration checklists and clinical documentation guides.







 Evan John
Evan John